Click HERE to access the RxIALTA study.
| Background |
Cardiovascular disease (CVD) is one of the leading causes of morbidity and mortality worldwide and in Canada accounting for nearly one third of the total deaths in both instances. The majority of CVD cases are caused by modifiable risk factors such as tobacco use, obesity, hypertension, hyperlipidemia, diabetes and physical inactivity. Inflammatory arthritis (IA), inclusive of rheumatoid arthritis (RA), psoriatic arthritis (PsA), ankylosing spondylitis (AS), gout and systemic lupus erythematosus (SLE) and cutaneous psoriasis are also recognized as an independent risk factor for CVD. It has been reported that the risk of myocardial infarction (MI), heart failure (HF) and CV death among patients with IA is 2–3-fold greater than in the general population.8-10 Similar numbers are reported for psoriasis. This increased CV risk reflects the combined impact of systemic inflammation, burden of traditional CVD risk factors and impact of certain medications (e.g. steroids, non-steroidal anti-inflammatories [NSAIDs], retinoids). An elevated risk of CVD can be identified early after the diagnosis, or even in the childhood, emphasizing the need for early efforts in CV risk screening. |
| Study Objectives |
Primary Objective: The primary objective is to determine the effect of a pharmacist-led intervention on CV risk in patients with IA and psoriasis. Secondary Objective: The secondary objectives are to determine the effect of a pharmacist-led intervention on the following factors: Blood pressure, Total cholesterol, HDL-cholesterol, LDL-cholesterol, HbA1c, Tobacco cessation (self-reported abstinence), Patient satisfaction |
| Study Design | A non-randomized prospective pre-post-intervention design. |
| Sample Size | For the primary outcome, we aim to detect a 21% relative reduction in CV risk between the pre-and-post intervention based on the findings of the RxEACH study (previously completed by our group). Given the expected reduction (21%), with 0.80 power, alpha of 0.05 and a SD of 17.8, the calculated sample size is 89 patients. Accounting for the risk of attrition from baseline to 6 months, we aim to recruit 100 patients. |
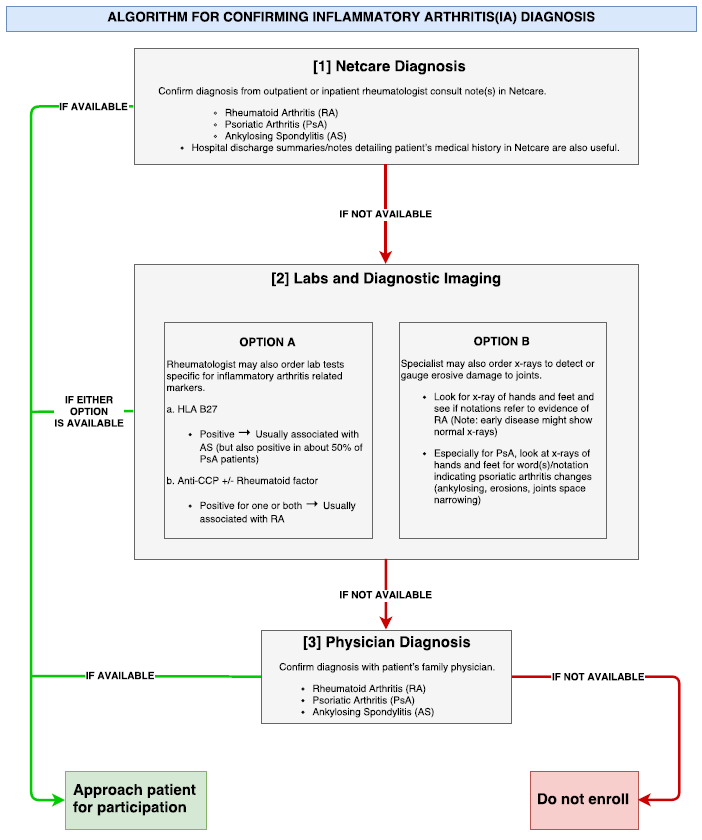
| Inclusion Criteria |
Adults (≥18 years of age) who have a physician-diagnosed inflammatory conditions including
|
| Exclusion Criteria |
Patients will be excluded if they
|
| Intervention |
All enrolled patients will receive the following:
|
| Outcomes |
Primary Outcome: The primary outcome will be the change in CV risk over a 6-month period. Cardiovascular risk is defined as the risk for future cardiovascular events (coronary heart disease [CHD], stroke, peripheral arterial disease [PAD]) as calculated by validated risk engines. The validated RxEACH CV risk calculator will be utilized to calculate CV risk. The calculator uses the most appropriate risk engine based on the patient’s medical history. Modified Framingham (Framingham risk score multiplied by 1.5), UKPDS , SMART risk score and Framingham will be used for patients with IA, diabetes, previous vascular disease or CKD respectively. In the case where a patient has more than one co-morbidity, the risk engine estimating the highest risk will be used. Secondary Outcome: The secondary outcomes will be the change over a 6-month period in: Blood pressure, Total cholesterol, HDL-cholesterol, LDL-cholesterol, HbA1c, Tobacco cessation (self-reported abstinence), Patient satisfaction |
| What This Study Adds | This is the first study to assess the effect of a pharmacist-led intervention on CV risk in patients with IA in the community pharmacy setting. It has a public health importance since it will provide CV risk assessment for a high risk population who otherwise will not receive such service. As well, it improves access to care in patients who are not affiliated with a family physician or those who see their family physician infrequently. Indeed, it has been reported that pharmacists see patients with chronic conditions more frequently than any other healthcare professional. As frontline professionals, pharmacists can be the first port of call to bring those patients back into the healthcare system. |
| Additional Resources |